HCSNet is funded by the Australian Research Council to promote research on human communication. I only got to go to the second day of the two-day conference (because I was cooking meals for 20 hungry rugby hopefuls the first day), but I saw a number of great presentations, including talks by Catherine Best, MARCS Auditory Laboratories, UWS, Beatriz Calvo-Merino, University College London, and Stephen Lord, Prince of Wales Medical Research Institute. I’ll blog soon on Dr. Calvo-Merino, one of the high points of the day, but today I want to make some notes on Prof. Lord’s fascinating research and talk.
Prof. Lord heads the Falls and Balance Research Group. Visit the group’s website for publications and some great information about risk factors for falling. At the conference, Lord discussed the group’s extensive applied research examining different factors that contribute to older people falling and experimental interventions to decrease the contribution of any single factor. The project has created a screening procedure for use by general practitioners to evaluate an older person’s likelihood of falling.
As regular readers know, I’m particularly interested in the way humans maintain equilibrium (see earlier posts, Kids falling down and Equilibrium, modularity, and training the brain-body, and Daniel’s post of some great parkour video, Free Running and Extreme Balance). In the longer of these posts (Equilbrium, modularity…), I specifically discussed how the ‘sense of balance’ is actually a much more complex synthesis of multiple sensory inputs, both exteroception (perception of the world) and interoception (perception of the self).
The problem of falling in older people
As the Falls and Balance Research Group website details, falls are a serious health issue for older people:
Falls are the leading cause of injury-related hospitalisation in persons aged 65 years and over and account for four percent of all hospital admissions in this age-group. Hospital admissions resulting from falls are uncommon in young adulthood but with advancing age, the incidence of fall-related admissions increases at an exponential rate. Beyond 40 years, the admission rate due to falls increases consistently by 4.5% per year for men (doubling every 15.7 years) and by 7.9% per year for women (doubling every 9.1 years). In those aged 85 years and over, the levels have climbed to 4% per annum in men and 7% per annum in women. Falls also account for 40% of injury-related deaths and one percent of total deaths in this age group.
Depending on the population under study, between 22-60% of older people suffer injuries from falls, 10-15% suffer serious injuries, 2-6% suffer fractures and 0.2-1.5% suffer hip fractures. The most commonly self-reported injuries include superficial cuts and abrasions, bruises and sprains. The most common injuries that require hospitalisation comprise femoral neck fractures, other fractures of the leg, fractures of radius, ulna and other bones in the arm and fractures of the neck and trunk.
With such serious potential consequences and such a clear trend towards increased likelihood as people age, Lord’s group fights the sense that falling is somehow inevitable. As he pointed out, some older people maintain stability, and the reasons that others lose stability can vary. The group’s Fall Assessment tests not only seek to predict the likelihood of falls (already pretty cool), they highlight which part of the complex system that regulates equilibrium is the weak link.
Understanding and disarticulating the equilibrium system
This last part — the differential evaluation of the various parts of the equilibrium system — is the dimension of Prof. Lord’s discussion that I find most interesting. The tests de-couple the contributions of visual system, vestibular system, proprioception, and musculo-skeletal strength to create a kind of ‘balance profile,’ showing clearly the difference between instability produced by failing strength, decreased leg sensitivity (from something like diabetes), visual problems (like glaucoma), and other issues. In my continuing attempt to model how cultural-behavioural variation affects the assembly of equilibrium, Lord’s group has come up with one of the most comprehensive discussions of the elements that contribute to a balance system. Even better, they’ve started to conduct research on where and how that system can start to come unstuck.
Lord’s presentation covered a range of issues, not all of which I can discuss, but I want to highlight a few, not only because they’re separately interesting but also because they give some sense of the subtle way that the research teases apart contributions to equilibrium. I don’t think it’s a satisfying statement to simply say that the equilibrium system is ‘complicated,’ and leave it at that; Lord’s group not only points out that the system is complicated, they also start to sketch out its parts, how they can go wrong, how disfunction can spread or compound across several components, and then how preventitive care or rehabilitation can address specific deficiencies.
One thing that Lord pointed out is that most falls were caused by slipping, tripping, or stumbling, not by dizziness or disorientation. That is, most falls seem to occur, not because the person loses awareness, but because some part of the mechanics of walking or standing goes wrong, and the person cannot recover quickly or effectively enough to stop from falling. The ‘margin for error’ when moving and standing decreases as reflexes slow and strength decreases, so a weakening of the balance system can’t be compensated. Starting to fall is normal; every step is a type of controlled fall. The question becomes why some people can’t stop themselves.
Problems in the equilibrium system
Vision issues:
As Lord pointed out, decreasing vision contributes to the chance of falls in older people, but it’s not just vision in a general way that most affects how people balance. In their screening, his research group specifically targets visual contrast acuity, depth perception, and peripheral vision, all of which can fall off more quickly than overall vision. Contrast vision is important because it’s what allows people to see changes in the height or angle of a surface, especially if the surface is a uniform color and material (like a concrete curb); obviously, decreased depth perception can severely affect mobility and even our attempts to stop ourselves from falling.
Peripheral vision can be diminished by conditions like glaucoma, Lord discussed, but what I was most interested in were his comments about bifocal glasses. Lord discussed how the design of bifocals actually exacerbates the problem with peripheral vision in the lower part of the visual field, precisely the area needed to navigate while walking. One of the interventions that the group recommended was simply giving older people who have indications that peripheral vision in the lower visual field might be an issue an extra pair of non-bifocal glasses — ‘walking glasses’ — inexpensively decreasing the chance of a severe fall that could result in hospitalization or incapacitation. (Just the kind of brilliantly simple preventitive treatment that might create huge savings in cost and suffering that we often wish our health systems did better.)
Interactions between senses:
In a series of experiments where the group shook the heads of subjects (sounds worse than it feels apparently), Lord and his team studied the vestibulo-ocular reflex, the way that the vestibular system stabilizes vision even when we are moving (that’s why the world doesn’t jump around visually when you’re running). They found that the vestibulo-ocular reflex can become less capable of compensating for movement as we age, although the variation in its degeneration was quite great. Some people don’t seem to lose much of the ability to compensate for movement in vision while others get quite lousy at tracking objects when on the move.
Leg and knee strength:
When Lord’s team did profiles of different people at risk of falling, some of them seemed to be disproportionately affected, not by vestibular problems or visual issues, but by leg strength problems. The variation in strength in the legs was enormous, according to some information he presented, and very simple things like lifting one’s leg high enough to clear an obstacle or change in surface height could be affected. Knowing that this was the ‘weak link’ in the balance system suggested relatively simple interventions to increase leg strength and flexibility. Most approaches to balance wouldn’t even consider ‘leg strength’ to be part of the system, but Lord’s team’s approach embraced the action part of the perception-action system and found that this was clearly where some people had their problems, especially after previous falls when injury had affected strength (so this might be a special risk factor in those suffering repeated falls).
Proprioception and sensitivity:
The falls research team tests proprioception and leg sensitivity in a number of ways. They found that certain conditions, such as diabetes, can severely affect the sensitivity of the lower limbs and feet and that some people become less aware of where their bodies are in space. Lord described how some people, when tested for vibration sensitivity at the knee, simply cannot feel the experimental stimulus, even when the vibration meter is set to its highest intensity. With numbed legs or feet, balance becomes a lot tricker, especially on uneven surfaces or when a person has a high degree of inherent bodily sway.
I asked Lord during the question time about de-afferentiation of the feet. That is, is it possible that, due to the wearing of hard shoes or thick soles, over time patients simply become desensitized to differences in pressure across the feet. In my own work, I’m wondering about the sensory impact of shoes. He said it probably wasn’t a serious factor, especially in comparison to the problems faced by those who were really losing all sensitivity in the lower limbs and feet. Fair enough.
But I still think that this may be an issue at certain levels of sensitivity, although it would be difficult to observe in a population that all wore shoes constantly and all spent most of their time walking on artificially smooth surfaces — in other words, our environment and clothing likely make us all a bit desensitized so the effect would wash out in the data. (I did notice that the Falls Prevention site does have assessment forms for footwear.)
Vestibular sensitivity:
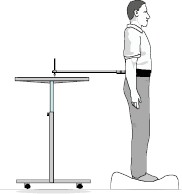
The screening test also checks to see how much people sway inherently while standing, and Lord reported that there is wide variety in this factor. The group tests people with an apparatus that looks like one of those ‘remote drawing’ machines; people stand attached to an arm that holds a pen. As they sway, they sketch out a little random figure on a sheet of paper. The group tests people on a solid surface and standing on a sponge pad to see how they respond to different situations. The resulting sway-o-grams pretty convincingly showed just how much inherent wiggle some older people had to contend with — it wasn’t just that they were getting worse at balancing, the inherent sway was making the whole system work harder to maintain vertical position.
The group has found that by increasing stimulation to the lower leg linked to swaying with passive stimulators decreases the amount of sway in older people, especially those who are losing sensitivity in their lower limbs. That is, if you create a way for people to feel when they are swaying on their calves (like lace up boots), they get sensory input that decreases the amount of swaying that they do, thereby decreasing the likelihood of falling down.
Conclusion
I’m not covering all the parts of the balance system that Lord’s team tests — for example, they do reaction time tests with a normal computer mouse and with a foot pedal in the long version of the test — but you get the idea. Overall, the wealth of information the group has produced and the comprehensive testing are a really admirable example of taking on a complex human perceptual-action system and patiently teasing out the different contributing factors. The approach seems to me to be harmonious with both a dynamic systems modeling of perception and action as well as an ecological approach to sensing.
The bonus, in this case, is that the robust modeling of the way that these different factors contribute to balance leads to very concrete interventions after a person’s specific ‘balance profile’ has been determined. That is, used well, this testing and diagnosis can really target why a person is becoming more unstable with time, and then address the specific weakness involved. Lord showed us some samples of profiles when he gave his talk, and it became quickly apparent that the preventitive exercises or treatment given to one patient wouldn’t help all the others. In all, the talk left me feeling that I had seen a role model, not only for integrative research, but also for application of the findings to improve people’s lives.
 Stumble It!
Stumble It!
Experimenting with inserting a Stumble function in this post seemed particularly appropriate…. GD
Further reading:
The group has a host of papers out on various dimensions of their research if you want more than you can get on the website (see their publications list, keep going down the page to find a complete list by individual topics). For example, you can check out:
Lord, Stephen R. 2006. Visual risk factors for falls in older people. Age and Ageing 35-S2: ii42–ii45. doi:10.1093/ageing/afl085 (abstract, pdf download) (Note: the whole supplementary edition is on research on fall-related fractures)
Menz, Hylton B., Stephen R. Lord, and Richard C. Fitzpatrick. 2006. A tactile stimulus applied to the leg improves postural stability in young, old and neuropathic subjects. Neuroscience Letters 406:23-26. doi:10.1016/j.neulet.2006.07.014 (abstract, pdf download)
Menz Hylton B., Meg E. Morris, and Stephen R. Lord. 2006. Foot and ankle risk factors for falls in older people: a prospective study. Journal of Gerontology: Medical Sciences 61A:866-870. (abstract, pdf download)
Voukelatos, Alexander, Robert G. Cumming, Stephen R. Lord, and Chris Rissel. 2007. Randomized, Controlled Trial of tai chi for the Prevention of Falls: The Central Sydney tai chi Trial. Journal of the American Geriatric Society 55:1185–1191. doi: 10.1111/j.1532-5415.2007.01244.x (pdf download)

Greg, what a great example. I was particularly impressed by the consideration of leg strength, the individual variability in sway, and on-going awareness of where your body is in space. Adds a lot to what we mean by “balance”, but also shows that we can focus on the specific processes involved in a research problem for great benefit, both for understanding and for intervention.
I’ve been reading Doidge’s The Brain That Changes Itself, and he relates an idea from Michael Merzenich about the decline in “gross motor control” as we age. To quote: “Aside from a failure of vestibular processing, this decline is caused by the decrease in sensory feedback from our feet. According to Merzenich, shoes, worn for decades, limit the sensory feedback from our feet to our brain. If we went barefoot, our brains would receive many different kinds of input as we went over uneven surfaces. Shoes are a relatively flat platform that spreads out the stimuli, and the surfaces we walk on are increasingly artificial and perfectly flat. This leads us to dedifferentiate the maps for the soles of our feet and limit how touch guids our foot control. Then we may start to use canes, walkers or crutches or rely on other senses to steady ourselves. By resorting to these compensations instead of exercising our failing brain systems, we hasten their decline.”
In other words, the argument is that the lack of diverse sensory input from our feet leads to the “use-it-or-lose-it” phenomenon in neuronal processing. This can create its own sort of “sensory weakness,” similar to the muscular strength weakness in the legs. And Doidge’s point about the emphasis on compensation, rather than re-training the under-used parts of the brain, is one he repeats throughout the book, as it works well with the break-it-down-into-pieces research approach (provided individual variation is also considered).
Not surprisingly, Chinese medicine, with its emphasis on accupuncture and accupressure, seems to have realized this sort of thing long ago. One particular “intervention” was to walk along a path of rounded but uneven stones, thus stimulating the feet (and thus the overall body). In the US, this has been adapted to a “cobblestone mat” that has been clinically shown to be an effective intervention for balance and for blood pressure in people over 60. For more info, see here: http://massagetherapy.suite101.com/article.cfm/reflexology_and_cobblestone_mats
Daniel —
So i think it’s official: everyone at Neuroanthropology has a copy of Doidge’s book. Paul and I were discussing it, too. And, yes, that whole discussion is why I asked Lord about deafferentiation of the feet. Thanks for reminding me of the ‘cobblestone mat’ example — I’ll have to include it in my eventual equilibrium chapter/paper (the one I’ll give at the AAAs if our panel gets accepted).
But overall, I think that balance is a great example — glad I’m not the only one. Since I’m also interested in the high-performance end of balance abilities, such as capoeiristas who achieve almost uncanny unbalance while walking on their hands and on Uighur kids who are taught to tightrope walk at a very early age, I’m intrigued by what other sorts of sensory input might also be brought into the ‘equilibrium synthesis,’ especially when some of the normal inputs are taken out of the equation. In other words, equilibrium is a great ability to deal with because, both in degenerate and exceptional forms, the ‘sense’ is making use of different sorts of sensory inputs, forms of self-monitoring, strengths, and behaviour patterns to keep the body balanced (which is itself a situatlonally defined standard, as different activities allow us to compensate in diverse ways — a tightrope walker has fewer action options to compensate for instability, for example).
But overall, it’s fun stuff. That’s why I’ve had such a great time getting stuck into it. Thanks, though, for the great reference. Lord’s research and work has been a great boost to my thinking, and I’ve barely scratched the surface on it. GD
The loss of peripheral vision is mentioned as a cause of falls in older people, but not the loss of central vision. Macular degeneration is increasingly a problem as we age and loss of central vision can also lead to falls in the elderly. “Walking” glasses are an excellent idea (though probably not so helpful for macular degeneration), as many optometrists only correct for reading and/or driving and cannot seem to comprehend that these visual corrections might create problems in depth perception which could lead to falls. Are there any optometrists out there with an interest in this area??
There is another cause to consider for falls in seniors called drop attacks. The bent base of the cranium and migration of the foramen magnum beneath the center of the skull predisposes humans to pressure conus type conditons in which the brainstem sinks into the foramen magnum. Pressure conus conditions were first noted as a result of spinal taps in which too much CSF was removed. A pressure conus compresses the brainstem and can result in loss of all vital funcitons and consciousness. The problem is that the brain floats in cerebrospinal fluid/CSF inside the cranial vault. Dilations in the subarachnoid space called cisterns are also stratigically located around the brainstem to provide additional support to keep it from sinking into the FM. Likewise in a similar condition called cerebellum tonsilar ectopia (CTE), which is also called a Chiaria condition, the tonsils of the cerebellum herniate into the foramen magnum. In any case, Chiari/CTE/pressure conus type conditons block the lowest and most important accessory venous outlets used by humans to drain the posterior fossa in the upright position. Chiari conditions consequently can cause hydrocephalus in the brian above the point of constriction and syrnixes in the central canal of the cord below. Blockage of these outlets also causes venous shifts and sluggish venous blood and cerebrospinal fluid flow out of the posterior fossa. This would affect CSF volume in the cisterns surrounding the brainstem. Except for the nose and eyes all of the other cranial nerves are located in the posterior fossa, including the eigth. Most of the CNs are located more ventrally on the underside of the brainstem toward the clivus. Either an increases or a decreases in CSF volume in the cisterns can compress these CNs. Additionally, an increase in CSF volume in the fourth ventricle would affect the flocculonodular lobe, which controls posture, coordination and balance and has close connections to the eigth CN. It also lies next to the tonsils of the cerebellum which are involved in CTE conditions. Recent studies show a significant correlation between cervical truama and Chiari conditions and Chirari conditons are known to cause drop attacks.