By Mary Kate McNamara, Emily Schirack, Dana Sherry & Amy Vereecke
Close your eyes. Imagine a crack addict. What do you picture? A wealthy man in an Armani suit and tie? Or a poor man clothed in baggy jeans; violent, dark and dangerous? Is she seated behind a mahogany desk on the 22nd floor of an office building in Manhattan or is she standing on a graffiti-covered street corner in East Harlem?
We know that a person’s drug of choice is influenced by his or her social status, from the high-powered lawyer with a penchant for powder cocaine to the pill-popping rock star to the alcoholic factory worker to the unemployed crack head. Here we will show something more important about a person’s relationship with drugs: an individual’s decision to use drugs is embedded in an unequal social structure, a social structure that produces unequal outcomes for drug users contingent on their social status.

By being poor, under-educated and of a low-status ethnic group, a person is at a greater risk for not only social marginalization, but becoming a victim of addiction (Baer, Singer & Susser 2003: 131). As David Courtwright argues in Forces of Habit, social inequality is promoted by the elite to maintain control over a minority group of laborers. By suppressing the lower classes in a cycle of substance abuse and addiction, the wealthy are able to increase their own power and profits. At the expense of people they deem inferior—simply because these people lack the material means to rise from their position—the elite sustain their authority. “Next to profits and taxes, the utility of drugs in acquiring, pacifying and fleecing workers proved to be their greatest advantage to the elites…” (Courtwright 2001:135)
In analyzing society’s abuse of drugs, Courtwright comments that “a pattern of drug use can become so entrenched in a culture that it is impossible to permanently suppress and delegitimate it” (Courtwright 2001: 199). This entrenchment is facilitated by a cycle of poverty, inequality and addiction.
Take Primo for example, a central figure in Philippe Bourgois’s book In Search of Respect. Primo is a Puerto Rican immigrant living in New York City’s Spanish Harlem. Without the necessary education or cultural capital, he is unable to find a legal job. Facing pressure to provide for his family, Primo turned to dealing crack. Feeling emasculated by his hopeless circumstances, Primo began to physically abuse his girlfriend. While the abuse gave Primp an outlet to assert his dominance and the drug dealing provided him with a source of income, his actions served to further entrench him in poverty. Drug dealing led Primo to drug addiction, which led him to squander his income on more drugs. Bourgois clearly shows that Primo’s social marginalization was deepened by his drug abuse, which in turn intensified his poverty and marginalization.

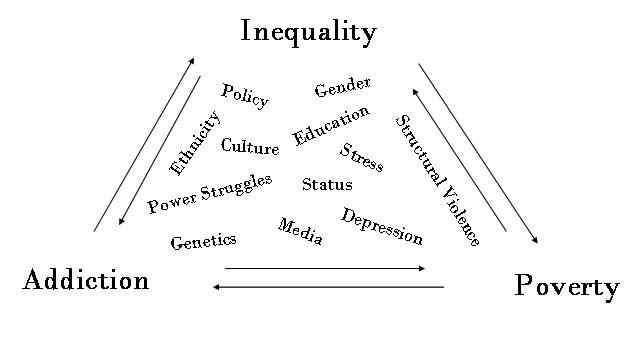
This cyclical component of poverty, inequality and addiction supersedes a person’s individual autonomy, making them victim to an incurable disease and a vicious cycle (see graph below). Epidemiological research has shown that individuals like Primo aren’t choosing their fates as an autonomous individual but rather having their fate dictated through a multifactorial combination of social, environmental, and biological components. Through their attempts to claw their way out of this cycle, people suffering from the hardships of social and economical marginalization can actually “become the actual agents administering their own destruction and their community’s suffering through turning to dealing drugs and embracing violence” (Bourgois 2003:145)
As Primo’s story demonstrates, many factors that plague the poor— stress of unemployment, depression, structural violence—contribute to addiction. At the same time, drug addiction contributes to both poverty and inequality, paralyzing the afflicted and rendering them unable to make positive changes or rise above their situation. For instance, a person reputed to be a drug addict or an individual with a drug-related criminal record is significantly less likely to be hired, and thus remains in the slums of poverty.
Ironically, one of the arenas where inequality is most visible is in the criminal justice system. Not only do whites comprise a larger portion of the drug users in the U.S., they actually outnumber blacks in the use of crack cocaine, a drug stereotypical thought of as a “black minority” drug (Husak 2002: 135). However, out of the 5 to 1 ratio of white to black drug users, there is a 2 to 3 ratio of incrimination of white to blacks. This statistic clearly shows a racial bias in drug criminalization. This bias has far-reaching consequences: estimates from the Bureau of Justice Statistics show that young black men are more likely to go to prison than to attend college.
Racial bias has also played a role in court cases where crack dealers were charged with much harsher sentences than cocaine dealers. Punishment for crack cocaine use and dealing (a drug associated with poor, black users) far outweighs punishments for identical crimes involving crack’s high-end counter part, powdered cocaine (associated with wealthy, white users). This inequality in law enforcement creates a “dual frustration” among minority populations living with drug problems and dealing with the harsh penalties of criminalization (Husak 2002: 136).
There are, however, strides being made to rectify the racial bias at work in the legal system. Recently, a Supreme Court ruling overturned a U.S. appeals court ruling that judges could not hand down lesser punishments on the basis that they disagreed with the wide disparities for crack and powder cocaine sentences. Nevertheless, these laws remain in place, contributing to the inequalities in drug use and the criminal justice system.
Of course, there is more to the story than unequal drug criminalization laws. Studies have shown that in low-income populations, children of parents who have been imprisoned are more likely to become criminals themselves (Husak 2002: 75). A child born to a drug-addicted mother in the inner-city is not going to receive the proper nutrition, education, or care that a child born to upper-middle-class parents will. As the child grows up, she sees her parents and peers suffer hardships due to discrimination, underfunded school systems, unsafe and run-down neighborhoods, minimum-wage employment, imprisonment, and poor health care. How are they supposed to rise above their parents’ limitations and the constraints of society? Continual experiences of racism, classism, and oppression combined with negative emotion and low self esteem among minority populations contribute to feelings of immobility within the social hierarchy (Baer, Singer & Susser 2003: 214).
Another arena in which inequality’s role in addiction is clearly visible is in the health care system. Inadequate health care has facilitated significant problems within the low-income population. Although impoverished people are more likely to have drug related health problems, they are less likely to receive treatment (Wood 2008). Black and minority populations receive less quality health care, slower care, and worse care than whites (Wood 2008). Only 17% of addicts who need treatment are capable of affording and receiving it. Programs to promote drug safety awareness are typically ineffective, including needle exchange programs and harm-reduction pamphlets instructing users how to properly clean needles with bleach (Bourgois 2002: 259).
Perhaps this graphic will help illustrate our points. The phrases in the middle are all factors that contribute to addiction, inequality, and poverty.
In order to break the cycle of drug addiction, the root causes need to be addressed. Social inequality is one of the biggest factors in that many addicts do come from low-income, low-opportunity backgrounds. Treatment needs to be readily available for all socio-economic backgrounds and the stereotypical profiling of an addict needs to be erased from the public mindset. As Elliott Currie suggests, “we need a multilayered approach: we need better treatment, more harm-reduction programs, selective decriminalization, more creative adolescent prevention efforts and much more…”
Works Cited
Baer, H., Singer, M., and Susser, I. Medical Anthropology and the World System. Westport, CT: Praeger Publishers, 2003.
Bourgois, Philippe. “In Search of Respect.” 1996.
Bourgois, Philippe. “Anthropology and epidemiology on drugs: the challenges of cross-
methodological and theoretical dialogue.” International Journal of Drug Policy 13
(2002): 259-269.
Courtwright, David. Forces of Habit. London, England: Harvard Printing Press, 2001.
Husak, Douglas. Legalize This! the case for decriminalizing drugs. New York, NY:
Verso, 2002.
“What is Addiction, and How Can We Treat It?” pbs.org. 4 April 2008.
.
Wood, Gina. “Unfair Treatment: Racial Inequality Produces Health Disparities.”
Journey to Wellness. 4 Feb. 2008. 4 April 2008. .

The New York Times has an excellent editorial today on the unequal patterns of drug-related arrests and convictions in low-income, minorty communities: http://www.nytimes.com/2008/05/10/opinion/10sat1.html?_r=1&hp&oref=slogin
Every family should educate their household on how addiction can ruin lives.